hi Swoop; the more I read into male pattern baldness stuff, the more I see a blurred boundary between anti-androgens meds and growth inducing meds.
I mean, I've always kept these 2 categories into 2 separate drawers in my mind, with labels: maintenance and growth stimulation.
E.g. metabolism of DHT in the follicles (both male pattern baldness and non-male pattern baldness ones) as one of the major signals for the follicle life cycle (at some point, an increase in DHT by local 5-alpha-reductase tells the follicle to enter catagen).
So, reducing DHT or blocking is only enlarging the anagen phase? (and what about the depletion of stem cells in the DP?)
So, I started being confused and thinking that it's always about having a longer anagen. Both classes of meds try to achieve the same goal...
What do you think? (I know, this is loosely connected to pilox, but.)
What do you mean exactly by this? Androgens are a prerequisite for Androgenetic Alopecia to occur, the same could be said for the androgen receptor.
Modulation of hair follicle cycling can be unrelated to the pathway chain of Androgenetic Alopecia. You can modulate hair follicle cycling in someone who doesn't have Androgenetic Alopecia too.
Take minoxidil or PGF2a (bimatoprost) for example. If you would give this to a norwood 1 non-Androgenetic Alopecia subject on his scalp it's highly likely that he will have increased hair counts too. Simply due to pushing telogen hair follicles into anagen and subsequently prolonging anagen or due to other hair follicle cycling alterations.
You can see this on body hair too with these compounds. Indeed both compounds can modulate the hair follicle cycle too in body hair. After all bimatoprost can be used to enhance the eyebrows/eyelashes and minoxidil can induce increased body hair growth, even hypertrichosis.
The difference is that they fundamentally don't do anything against the pathway chain of Androgenetic Alopecia. Let me give you an example. You can take a subject who is balding and give him minoxidil to use on his head. He will show increased hair counts simply because the compound is altering the hair follicle cycle. You also give him some minoxidil to use on his beard. He will have better hair growth too. However over time his hair on his scalp will start suffering because you are fundamentally doing nothing against the damage and he will fall below baseline. His beard however won't suffer and as long as he is applying the stuff he is changing the hair cycle there and he will stay above baseline there.

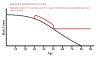
Works like that on average. Finasteride will make you stay at least above baseline in most subjects for a long period of time. Minoxidil won't and this reflects in the studies done on minoxidil too where subjects will initially have increased hair counts but will fall back to baseline within 2 years. Now there are some (weak) studies done by Olsen for instance where minoxidil can let someone stay above baseline for more than 5 years. Yeah well guess what man if you would put minoxidil on Brad Pitt his scalp it would give him hair counts above baseline probably for over 10 years lol. This is logical as he wouldn't suffer from Androgenetic Alopecia, same as the beard hair. It's also important in some studies where the measurement has been taken (on what part of the scalp). Was it on a very sensitive area of subject in the frontoparietal region? Or somewhere in the mid scalp where the hair follicles of the subjects weren't genetically programmed to succumb aggressively?
Now you could hypothesize that minoxidil might actually do something against the pathway chain of Androgenetic Alopecia itself. For instance
here is a study that mentions that it may suppress androgen receptor related functions. In that sense it might "control' a (tiny) part of the damage too of Androgenetic Alopecia. But how much weight should we put to something like that. Probably not much as evidenced by the studies of minoxidil.
Currently we only have two targets to follow to disrupt the Androgenetic Alopecia chain completely and that is either acting on androgens or the androgen receptor. The latter is very hard with current drugs but the former is easy through castration.
Now you could also hypothesize that you can act in damage control of other factors that are implicated in the Androgenetic Alopecia chain. A simple schematic hypothetical scenario would look like this
Androgens > AR > ... > ... > PGD2
Androgens > AR > ... > oxidative stress
Now in this situation you might act on PGD2, through for instance using a DP2 antagonist or using a strong anti-oxidant to deal with "part" of the damage of the pathway chain of Androgenetic Alopecia to slow down the progression. In this situation you aren't necessarily modulating hair follicle cycling but dealing with the pathway chain. This is pure hypothetical though, the best is to deal with androgens. That being said prostaglandins are implicated in modulation of hair follicle cycling too. It's dynamic as you can see. We need to understand Androgenetic Alopecia more.
Multiple factors can modulate hair follicle cycling btw. For instance some people are born with genetic defects. Like VDR mutations, EDAR, HR (hairless).. You can see in these people that they often suffer from full or partial alopecia in their life. You could say that these factors are necessary for proper hair follicle function.
Similarly you have some compounds that induce heavy hair loss like a SHH antagonist.
Also like I mentioned in the above generally telogen hair follicles are very responsive to environment stimuli. In some studies for instance it has been shown that a simple ethanolic vehicle can lead to increased hair counts lol. Something like cyclosporine will also modulate hair follicle function, resulting in hypertrichosis. I
Another example would be someone suffering from thyroid disease which could lead to hair loss.. Well if you look at the following studies;
Neuroendocrinology of the hair follicle: principles and clinical perspectives
The human hair follicle (HF) is an exquisitely hormone-sensitive mini-organ that undergoes cyclical remodeling. It is also a source and target of numerous neurohormones, neuropeptides, and neurotransmitters that regulate HF growth, pigmentation, remodeling, immune status, stem cell biology, and energy metabolism. Indeed, organ-cultured human scalp HFs can be utilized to identify ‘novel’ clinically relevant functions of major neuromediators. This is pertinently illustrated by the discoveries of: (i) thyrotropin-releasing hormone (TRH) as a hair growth and pigmentation stimulator; (ii) TRH and thyrotropin (TSH) as potent promoters of mitochondrial activity and regulators of keratin expression; and (iii) prolactin as an epithelial stem cell modulator. Thus, HF neuroendocrinology affords insights well beyond hair growth and dermatoendocrinology, uncovering new translationally relevant neuroendocrinology principles and novel therapeutic targets.
Pituitary thyroid-stimulating hormone (TSH) regulates thyroid hormone synthesis via receptors (TSH-R) expressed on thyroid epithelial cells. As the hair follicle (HF) is uniquely hormone-sensitive and, hypothyroidism with its associated, increased TSH serum levels clinically can lead to hair loss, we asked whether human HFs are a direct target for TSH. Here, we report that normal human scalp skin and microdissected human HFs express TSH-R mRNA. TSH-R-like immunoreactivity is limited to the mesenchymal skin compartments in situ. TSH may alter HF mesenchymal functions, as it upregulates alpha-smooth muscle actin expression in HF fibroblasts. TSH-R stimulation by its natural ligand in organ culture changes the expression of several genes of human scalp HFs (for example keratin K5), upregulates the transcription of classical TSH target genes and enhances cAMP production. Although the functional role of TSH in human HF biology awaits further dissection, these findings document that intracutaneous TSH-Rs are fully functional in situ and that HFs of female individuals are direct targets for nonclassical, extrathyroidal TSH bioregulation. This suggests that organ-cultured scalp HFs provide an instructive and physiologically relevant human model for exploring nonclassical functions of TSH, in and beyond the skin.
It's not such a surprise either that someone with shitty thyroid function in rare cases can have hair loss too due to hair follicle cycle modulation of disrupted TSH levels. The hair follicle is a complex mini-organ.
Examples go on... I can't give you an exact calibrated answer on this all though. We'll need to know more about Androgenetic Alopecia. It's important to prevent as much damage from happening in Androgenetic Alopecia though.


")