- Reaction score
- 498
Are we sure that it doesn't build up systemically long term? 15 percent is negligible, even saw palmetto doesn't inhibit that less DHT

To understand it better, for how long have you been using 0.1% non-liposomal dutasteride and how often because it seems like build up didn't occur in your caseBuild up could happen, half life is 4 weeks.
That is why I apply once a week max, sometimes once every 2 weeks, sometimes every 10 days, I don't have sides so I don't care.
Have you ever used it once per two weeks for a longer enough of time to judge whether once a week is way better than twice a week?Not sure. 2 months or 3 months.
I don't keep exact dates.
If it's Liposomal or not it doesn't matter. Completely irrelevant when it comes to build up
I was once obsessed with liposomal finasteride which is a huge drop from what I've researched or saw anecrodally. That suggests liposomal makes little to no difference to keeping the substance on scalp more. I assume it's the scheduling that makes dutasteride side effect free. Ketoconazole, spironolactone don't give expected sides topically and both had studies that show they go systemic at a negligible rate, both of them have close molecular weights to dutasteride so maybe dosing and frequency and give benefits in a very safe fashionTo anyone reading the thread, liposomal or not turned out to be irrelevant in Mustang's case with regards to build-up, but there are many other reports of people trying topical dutasteride with a regular vehicle (non-liposomal) and getting side-effects, so for those cases the type of vehicle is actually very relevant. Something to consider if you're going to use non-liposomal topical dutasteride.
Great! Could you share the measurement that shows a %80 reduction in scalp dht with us? (Or send me in private if you prefer that)I'm going to be running some plasma DHT tests with
Topical Dutasteride 0.05%, 0.1% and 0.5%
On scalp I already know that 0.1% reduces 80% while plasma going down just 15% (which to me is nothing). It went down 20% for another user but he was applying 1.5ml thus 0.1,5% essentially. Still anything below 25% is nothing DHT wise.
I assume 0.05% will be close in scalp reduction but probably leave plasma intact.
Will report once I have the measurements back.
It's oral. Topical may be better in this case even though usually it isn'tGreat! Could you share the measurement that shows a %80 reduction in scalp dht with us? (Or send me in private if you prefer that)
I just skimmed through a couple studies and the reduction in scalp dht when taking 0.5 dutasteride a day seems to be about %50
I was once obsessed with liposomal finasteride which is a huge drop from what I've researched or saw anecrodally. That suggests liposomal makes little to no difference to keeping the substance on scalp more. I assume it's the scheduling that makes dutasteride side effect free. Ketoconazole, spironolactone don't give expected sides topically and both had studies that show they go systemic at a negligible rate, both of them have close molecular weights to dutasteride so maybe dosing and frequency and give benefits in a very safe fashion
Thank you. I always assumed 4 week half life was based on 0.5 mg generally approved dose but hopefully it's wrong. Please update us as I couldn't find anything for the last week tooIf it turns out that a liposomal vehicle reduces systemic absorption (even if only by a small amount) I would argue in favor of it because it allows you to maximize the amount of dht inhibition in the scalp in relation to the rest of the body. That being said, you raise an interesting point.
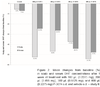
As far as I know there's no single dose data on dutasteride, but we can consider the following graph from a study on finasteride:
View attachment 145043
Possible problems/unknowns:
- If I remember correctly, 0.5mg of dutasteride is comparable to 1.5mg of finasteride in terms of dht-inhibition (someone correct me if I'm wrong).
- The graph shows it takes roughly 7 days for dht in plasma to return to baseline after finasteride, with higher dosages taking slightly longer.
- This graph is based on oral administration. So if 1.5mg finasteride/0.5mg dutasteride enters the bloodstream, it will take the body around 10 days to recover and return to baseline.
- It actually doesn't seem that far-fetched that an appropriate dose of topical dutasteride would result in significant dht-inhbition in the scalp, while the body clears the smaller part of it that goes systemic.
There does seem to be merit to the idea of applying single doses and waiting for it to clear from the body, because the effects seem much more manageable and predictable. Accumulation becomes less of a problem.
- Dutasteride has a different half-life, but as I've mentioned several times, I think it's halflife is dose dependent. So it's not necessarily 4 weeks. With a single dose I expect the half-life to be much lower. I'll dive into the literature when I have time to see if I can figure out what the halflife would roughly be at a single dose. I'm also still not sure how the half-life actually relates to any of this. With finasteride it seems largely irrelevant, because the actual amount of time it binds to enzymes is much longer. The rate at which the body produces new 5ar enzymes seems to be more important? (If anyone can shed light on this, please do).
- If plasma dht returns to normal after roughly 7 days, does that also mean that scalp dht has returned to normal after roughly 7 days?
- If it does, that might mean that dht-levels in the scalp are in a continuous state of change, being heavily reduced shortly after dosing, and being near-normal right before the next dosage. I imagine constantly changing dht levels in the body could have negative consequences, but I wonder whether that also applies to the scalp (aside from the fact that the hair follicles become progressively more vulnerable, until the next dose at least).
- If it doesn't, does that mean that a larger amount of dutasteride will bind to enzymes elsewhere in the body, because the scalp is already partly saturated?
Thank you. I always assumed 4 week half life was based on 0.5 mg generally approved dose but hopefully it's wrong. Please update us as I couldn't find anything for the last week too
To anyone reading the thread, liposomal or not turned out to be irrelevant in Mustang's case with regards to build-up, but there are many other reports of people trying topical dutasteride with a regular vehicle (non-liposomal) and getting side-effects, so for those cases the type of vehicle is actually very relevant. Something to consider if you're going to use non-liposomal topical dutasteride.
This doesn't make much sense to me since Liposomes are there to enhance absorption, not prevent it.
I am not using a regular vehicle (it has no alcohol)
I think you are absolutely right about the frequency being key here. I overdosed massively every 10 days applying 50MG of Dutasteride, that is 100 times the dose and my plasma DHT was still there.
And I just found this in a patient leaflet for Combodart (some kind of medication which combines dutasteride and something else):
Elimination
Dutasteride
The elimination of dutasteride is dose dependent and the process appears to be described by two elimination pathways in parallel, one that is saturable at clinically relevant concentrations and one that is non saturable.
At low serum concentrations (less than 3 ng/mL), dutasteride is cleared rapidly by both the concentration dependent and concentration independent elimination pathways. Single doses of 5 mg or less showed evidence of rapid clearance and a short half-life of 3 to 9 days.
At therapeutic concentrations, following repeat dosing of 0.5 mg/day, the slower, linear elimination pathway is dominating and the half-life is approx. 3-5 weeks.
What is the current vehicle do you use?This doesn't make much sense to me since Liposomes are there to enhance absorption, not prevent it.
I am not using a regular vehicle (it has no alcohol)
I think you are absolutely right about the frequency being key here. I overdosed massively every 10 days applying 50MG of Dutasteride, that is 100 times the dose and my plasma DHT was still there.
I found the study in question: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2014202/. A couple of excerpts to illustrate what I meant:
The parameters of the final model are displayed in Table 1. After a short lag-time, the absorption of GI198745 was rapid, followed by a brief distribution phase. The pharmacokinetics of GI198745 showed an unusual profile, where a high volume of distribution (511 l) and a low linear clearance (0.58 l h−1) combined to give a half-life of up to 5 weeks at high concentrations. As concentrations declined towards Km (0.96 ng ml−1) the proportion eliminated by the relatively rapid saturable elimination pathway, with a maximum clearance of 6.2 l h−1 (calculated as Vmax/Km), increased and the half-life reduced to about 3 days.
Possible explanations for the nonlinearity include a low capacity metabolic pathway or saturable biliary excretion. Another possible explanation for the nonlinearity could be irreversible binding of GI198745–5α-reductase and subsequent breakdown, a process that would be saturated as the amount of free 5α-reductase decreases.
View attachment 145044
I would assume (and I may be wrong, I'm not an expert) that we're at the lowest end of the spectrum because're only applying once a week, of which only a minor part will go systemic. Maybe someone more knowledgeable than me is able to use this article's model to calculate the half-life for this particular situation. In any case, it does seem to me that dutasteride's halflife when dosing once a week is at the very least much shorter than five weeks, and possibly even shorter than three days. If so, then the amount of time it takes the body to produce new enzymes would be the main factor to consider, rather than the half life, right? And that would make it more comparable to finasteride, at least in terms of drug duration.
Yeah, obviously it oral.It's oral. Topical may be better in this case even though usually it isn't
Are there any logical explanations for the topical version to inhibit more scalp dht than oral?
Its a bit unfortunate though that Mustang seems to avoid important questions asked in this thread (not only by me).